
Menu
Robotic Nephron Sparing Surgery for Renal Tumors
Robotic Nephron Sparing Surgery for Renal Tumors
(Excision of only the diseased part of kidney)
In order to perform an open nephrectomy (in the language of medicine, total removal of kidney is called nephrectomy), a surgical incision that can reach up to 35-40 cm is being made (Image-1). Especially during excision of large tumors, sometimes 12th rib has also to be removed through the same incision. There will be long-term pain and numbness around surgical site due to the damage caused to muscles and nerves while making this large surgical incision. Besides, recovery will be late accordingly. In addition to these, a hernia that might be occur after the surgery will also cause discomfort and affect patient’s life quality.
After USA and European countries, nowadays laparoscopic kidney surgery has become a standard surgical procedure in our country, too. However, thanks to the technologic advantages offered to urology by daVinci Robot, robotic surgery in treatment of renal cancers has come to the fore. But in terms of efficiency, there is not a significant difference between Radical Nephrectomy (which is total removal of kidney) and Robotic Surgery or Conventional Laparoscopic Surgery performed for kidney tumors. However, thanks to Robotic System our patients can be offered a surgery performed using 10-15 times magnified, 3 dimensional high-definition vision system, and robotic arms which eradicate any hand tremors and can move in many directions like hand.
The main surgery during which Robotic Surgery technique provides especially technical advantage is Nephron Sparing Surgery for Renal Tumors, which is also called Partial Nephrectomy or Nephron-Sparing Renal Tumor Excision.
Tiny filtering systems in our kidneys are called nephrons, and each of kidneys contain nearly one million of them. And the surgical technique during which only the cancerous tumor is removed, so nephrons are preserved is called ‘’Nephron Sparing Tumor Excision’’.
What are the Advantages of Robotic Radical Nephrectomy?
- Since it is performed in the extraperitoneal area, there is no risk of bowel injury
- Short hospitalization period and fast recovery
- Less pain and less need to take pain killers post-operatively
- Being able to carry out daily routines in a short time
- Due to small surgical incisions, better cosmetic results
- Three dimensional, high definition display
- Magnified imaging
- Surgery via robot arms that eradicate tremors
- Performing the operation via robot arms inserted into body, that are capable of easily maneuvering in 7 directions and multiple angles like hands.
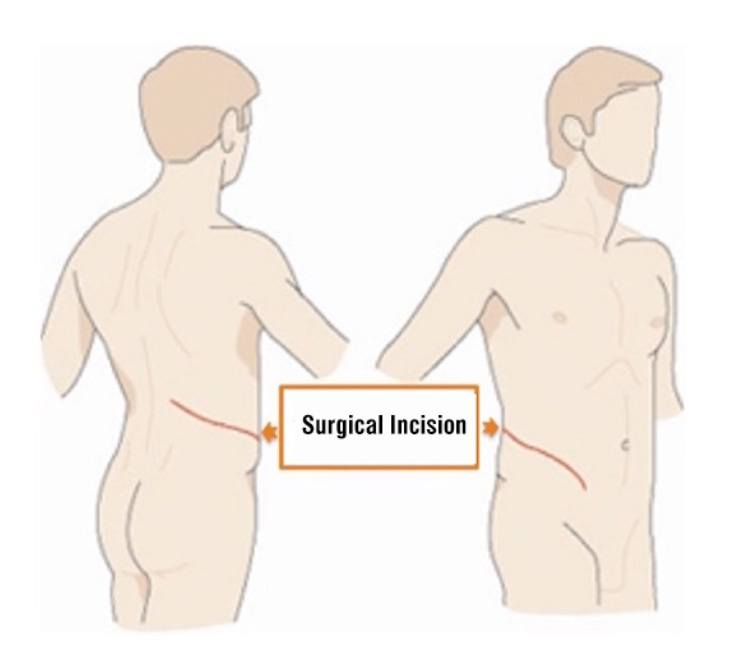
Image-1: Open Nephrectomy – During open kidney surgery, 3 layers of muscle composing abdominal wall are cut through consecutively with a big flank incision. As a result of incising these muscles, patients feel serious pain and recovery period will be longer because of the scar size.
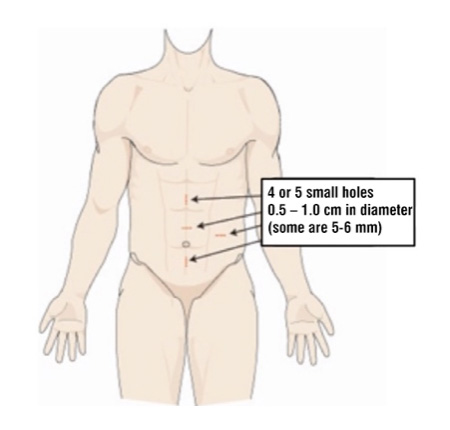
Image-2: Robotic Partial Nephrectomy – Locations of the small holes opened on anterior abdominal wall during robotic or laparoscopic kidney surgeries. Robotic technology, with the advantages it brought, has an important place in partial (nephron sparing) surgery.
What is Robotic Partial Nephrectomy?
In order to watch related surgery videos after reading this part, please CLICK HERE.
This technique can be used especially for renal tumors that are 4cm or smaller in diameter, depending on their locations in kidney. Our aim in here is removing only the cancerous tumor tissue and leaving healthy part to the patient, while keeping the cancer under control. However, thanks to our latest experiences in laparoscopic and robotic surgeries, now we are able to partially excise renal masses that are 6-8 cm in diameter, while preserving the remained healthy part of kidney.
In order to watch extremely challenging excision of a huge mass (8 cm in diameter) that compresses main renal veins and collecting duct system of the kidney, and how the healthy kidney tissue is being preserved at the same time via Robotic Surgery, please CLICK HERE.
In the last 10 years, surgical practices in laparoscopic technique have broadened seriously: once only ablative surgeries were being performed, during which the unhealthy tissue was removed totally; but now much more complex reconstructive surgeries (excision of unhealthy part, and mending the gap) are being performed. The standard practice in localized kidney tumors that can be operated with organ (kidney) sparing surgery technique is the open partial nephrectomy.
Thanks to increasing experience in intracorporeal suturing (suturing and knot-tying inside the body) and advanced laparoscopic vessel devices used during laparoscopic technique, it has become easier to perform partial nephrectomy via laparoscopic technique in selected patients. Therefore, today even in small tumors, we can perform a laparoscopic renal tumor surgery through 3 or 4 holes (one is 1.2 cm, the other 1.0 cm and one or two more 0.5 cm) by leaving healthy tissue behind, while excising only the tumor. In the long-term and medium-term scientific follow-ups carried out for cancer control, laparoscopy has testified itself as a technique that can be used securely and conveniently. However, nowadays after meeting advantages of daVinci Robotic System, urology practitioners have started to benefit from these advantages offered by daVinci Robotic System for repairing tissue gap, injured vessels and damaged urinary canals, which occur following the excision of tumorous part in kidney.
While tumor tissue is being excised and the part left behind is being repaired by sutures, renal artery is clamped in order to prevent bleeding. Kidney can not have blood supply during this period (kidney can stay 15-20 minutes without blood flow). Surgeon excises the tumorous tissue without posing any risk in terms of cancer control, then repairs the damages in this area. A surgeon must have extensive experiences in laparoscopy and robotic surgery in order to perform these steps. Because, laparoscopically repairing the kidney tissue that is extremely bloody during this period is a very hard technique to master. However, an experienced surgeon performing laparoscopic technique while benefiting from the technologic advantages of daVinci system can overcome these challenges with ease, thanks to this technologic assistance.
Technologic advantages provided by daVinci system, thanks to which an experienced laparoscopic surgeon can surmount the challenges while racing against time during partial nephrectomy, can be listed as follows:
- With daVinci system, borders of the tumorous tissue can be marked with assistance of 3-dimensional (3D) display system, instead of 2-dimention laparoscopic technique offers.
- Thanks to 3-dimensional high-definition display, tumors can be excised with great depth perception.
- Suturing is performed via robot arms, with no tremor.
- With use of robot arms that are capable of 540 degrees of articulation, the area tumor is excised from can be quickly sutured no matter where the tumor is located, thanks to depth perception offered by this system.
These can be listed among certain indications for performing Partial Nephrectomy for Renal Cancers:
- Synchronous bilateral kidney cancer cases
- Patients with solitary kidney (only one kidney) diagnosed with kidney tumor (unilateral renal agenesis or previous contralateral nephrectomy)
- Tumor existence along with a malfunctioning or non-functioning second kidney.
These can be listed among uncertain indications for performing Partial Nephrectomy for Renal Cancers:
- Having diseases that may pose a risk for kidney impairment in the future (for instance- diabetes, high blood pressure)
- Small tumors, which are inclined to extend outwards
- Renal cancers diagnosed at a young age
- Family history of renal cancer (genetic susceptibility)
Treatment of prostate, bladder, kidney and testicular cancers with robotic and laparoscopic surgery in urology
Our Clinic

- Hacı adil cad. Zerrin sokak, No:2/2 Levent, 34330 Beşiktaş İstanbul Turkey
Prof. Dr. Tibet Erdoğru – Urology & Robotic Surgery | Data Privacy | Cookie Policy