
Menu
da Vinci Robotic Surgery
Robotic & Laparoscopic Surgeries:
what is the differences ?
- What is Laparoscpic surgery?
- What is Laparoscopic Radical Prostatectomy?
- What is “Robot Assisted Laparoscopic Surgery” (Robotic Surgery)?
What is laparoscopic surgery?
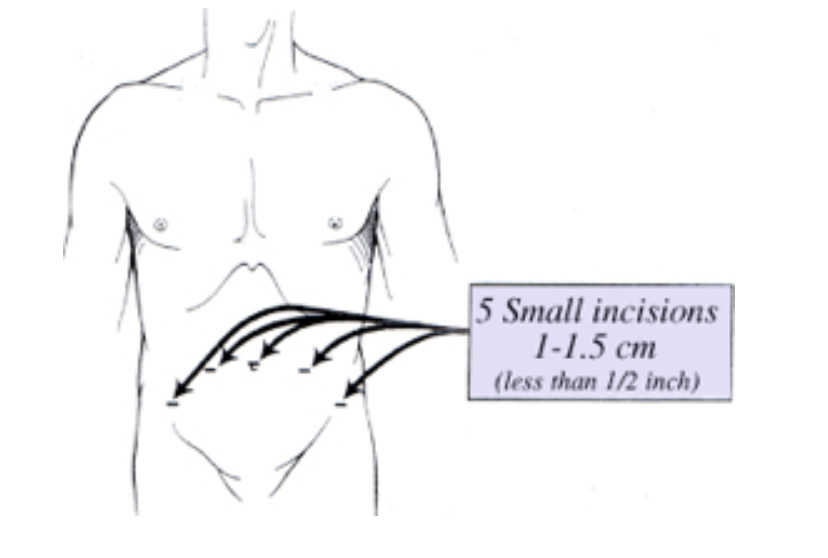
As in Turkey, laparoscopic urological surgery stories gained importance and started to be applied after 2000s. Laparoscopy is a technique that is performed by a camera placed from 4 or 5 tiny holes (0.5-1 cm) and long-thin surgery equipments instead of large surgery cuts (about 20 cm) in surgical treatment of intraabdominal or intra pelvic organs (Figure 1) Also, a high definition digital telescopic camera system with 1.5 cm placed in one of tubes that provides to view organs to be operated such as kidney, prostate, urehtra and surrenal gland is used. The image in the body is reflected to a screen by this telescope-camera system and the operation is performed with this 10-20 times enlarged view of normal. Because of these tiny holes used in laparoscopic surgery provides less discomfort and more aesthetic appearance after the laparoscopic surgery according to large surgery cuts in open surgery. Operation pain and use of pain killers, hospitalization and recovery period decreases ver much after the surgery with laparoscopy. Laparoscopic surgery is performed under general anesthesia like open surgery. Although laparoscopic surgery is a technique that provides great convenience according to open surgery in terms of patients, application requires large experience. Prof. Dr. Tibet Erdogru has a great experience about laparoscopic surgery with surgeries over 600 and laparoscopic radical prostatectomy surgery over 300.
Figure-1: Laparoscopic surgery is performed by placing thin surgical tools from tiny holes.
What kind of benefits will be gained by laparoscopic surgery?
Many determined benefits are provided in researches in terms of patients when compared with open surgery.
* Less post operational pain
* Less bleeding
* Less hospitalization period
* Acceptable aesthetic apperance/small scar
* Rapid return to daily activity
* Better continence and erectile function rates
Laparoscopic nad Robotic surgical technique in treatment of prostate cancer:
What is Laparoscopic Radical Prostatectomy?
Traditional open radical prostate surgery that provides removal of prostate completely used to be applied to patients whom limited prostate cancer is detected. Laparoscopic radical prostate surgery has started to be applied especially since 2000. In this approach, prostate is removed completely and after removal of prostate, bladder neck and urinary tract (urethra) are sewn by making them corresponding. During removal of prostate, green courage in Figure -2 is protected and provides to hold the urine.
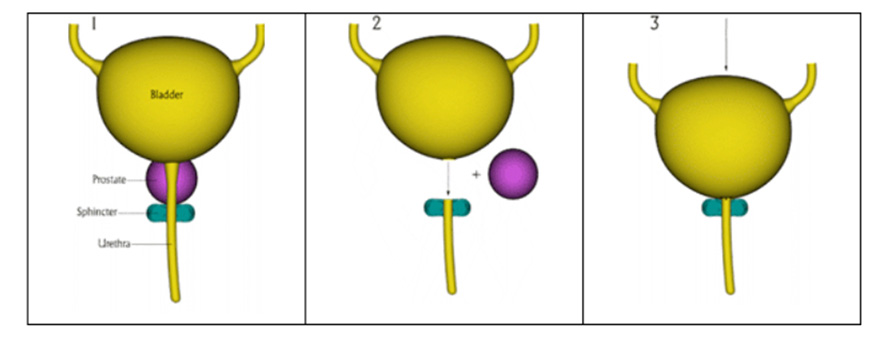
Figure-2:In radical treatment of prostate cancer, as seen in this diagram, after prostate is removed urinary tract is sewn to the bladder neck from outer courage level and continuity of the channel is provided.
For laparoscopic prostate surgery conventional (classical- not robot assisted) 5 small holes (between 5-10 mm) should be opened (Figure-1). One of these holes (10 mm) are opened from umblicus and it does not ruin the aesthetic view. The other two 10 mm holes are opened on both down-side of umblicus and 4-5 fingers from umblicus and the last two 5 mm holes are opened to two fingers upper-inner part of upper side of pelvis. However, thicker and 6 trochar are placed in robotic surgery. Carbondioxide gas is given to the body from a pipe channel (port, trochar) placed from the hole in umblicus. Abdomen is pushed to sides and up by this gas and intraabdominal area may be imaged as fifteen times enlarged and provides us to work comfortably. After required evaluation, surgical process for surgical prostate starts.
In Extraperitoneal laparoscopic or robotic radical prostatectomy, the operation is performed without piercing the peritoenum membrane, covers intraabdominal organs (such as intestine, liver, spleen). But in robot assisted laparoscopic radical prostatectomy, applied in our country and all over the world, Access is performed from abdominal membrane, thus transperitoneal. With this transperitoneal way, intestines are directly contacted and intestines are exposed to direct contact of instruments are given into the abdomen. Also, the patient is laid 45-60° upside down to keep intestines separate from surgical area. This causes increase of heart load and increase of blood load to kidneys. The Extraperitoneal Robotic Technique that Prof. Dr. Tibet Erdogru applies, same surgical intervention is performed out of peritoneum (extraperitoneal). With this extraperitoneal approach, no contact with intestines, intestines are nor exposed to high intraabdominal pressure directly and only 10-15° upside-down position is given to the patient. Therefore, no overload in heart and kidney and patients start to eat fluid food in the same evening after the surgery. However, in transperitoneal approach, start of intestinal motility may take two days.
- Hospitalization period after the surgery is 1 or 2 days. 95% of patients go to home in second day after the surgery.
- When compared with conventional open surgery, less blood loss arise during the surgery. Paralelly blood transfusion rate is very low (2-3% in laparoscopic surgery, 40-45% in open surgery)
- The pain requires minimal painkillers during hospitalization period, also less pain killer use is in question after discharge.
- If there is no recovery problem within the first week after the surgery, the catheter placed into the urinary tract is taken. This period ranges between 14-21 days in open surgery.
- 90% of patients return to their routine work in the two weeks after laparoscopic or robotic radical prostate surgery.
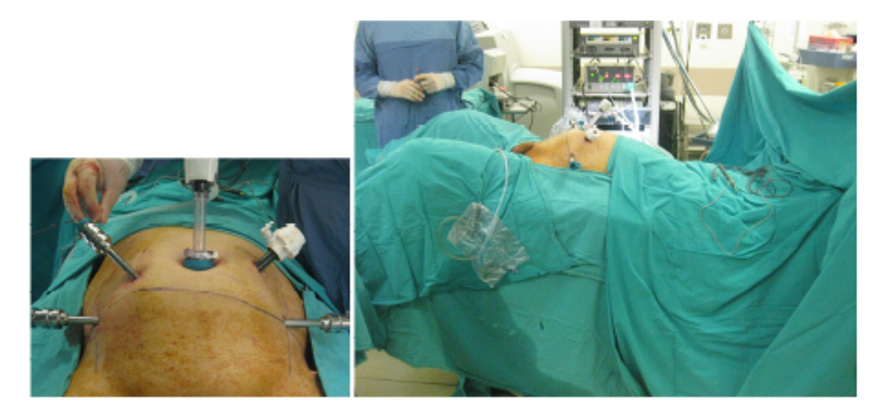
Figure-3: Performing extraperitoneal radical surgery (radical prostatectomy) which is prostate cancer surgery of laparoscopic and robotic surgeries from thin tubules without opening large cuts with minimal upside down Trendelenburg position
Are you a suitable member for laparoscopic or robotic prostate surgery?
If the cancer in your prostate is limited and not diffused out of the organ and you do not have an additional serious disease, you are candidate for surgical treatment.
If beam therapy was applied to the prostate cancer outside or inside (brachitheraphy) and cancer control cannot be provided, you are not a good candidate for surgical treatment.
If you have an uncontrolled blood disease, you are not an appropriate candidate for prostate cancer surgery. Except these two points, laparoscopic radical prostatectomy is applied to all patients.
What are side effects or complications?
Evaluations done till now show that urinary incontinence and penil erectile function disorder frequency is less in laparoscopic and robotic prostate surgery. If you are younger than 70 and double nerve protective technique is applied, you can perform your sexual function with 95% rate without additional treatment after bilateral intrafascial nerve-sparing approach with robotic surgery.
What is “Robot-assisted laparoscopic surgery” or “da Vinci Robotic Surgery”?
“Robotic Surgery” phrase is not used in scientific arena in United States of America. The term used for this technique is “Robot Assisted Laparoscopic Surgery”. Actually the technique called robotic surgery is basically laparoscopic surgery except some advantages and disadvantages. Therefore, those who apply Robotic surgery use “Conventional-Classic-Laparoscopy” term for their comparison. Because the technique they apply is “Robot Assisted Laparoscopy”.
Basic steps of surgical process, applied to the patient, are similar in “Robot Assisted Laparoscopic Surgery”. As shown in Figure-1, -2 and -3, the surgical process is performed with robotic arms with 3D HD telescope and robotic arms containing articulated surgical tools.
The most important differences between “Robot Assisted Laparoscopy” and “Conventional Laparoscopy”, providing multi directional movement to 3 ways with instruments fixed to the robotic arms and HD 3 dimensions in the view via a tool (robot) between the physician and the patient.
Robotic surgery allows doctors to perform many types of complex surgical procedures with more precision, flexibility and control than is possible with conventional techniques.
The most widely used clinical robotic surgical system includes a camera arm including two telescopes for 3D view and mechanical arms with surgical instruments attached to them. The surgeon controls the robotic arms while seated at a computer based console near the operating table. The computerized console gives the surgeon a high definition (HD), magnified (15x), 3D view of the surgical side.
The major benefits of robotic surgery include:
- Fewer complications, such as surgical site infection
- Less pain and less blood loss
- Shorter hospital stay and quicker recovery
- Smaller, less noticeable scar tissue abdominal wall
Treatment of prostate, bladder, kidney and testicular cancers with robotic and laparoscopic surgery in urology
Our Clinic

- Hacı adil cad. Zerrin sokak, No:2/2 Levent, 34330 Beşiktaş İstanbul Turkey
Prof. Dr. Tibet Erdoğru – Urology & Robotic Surgery | Data Privacy | Cookie Policy