
Menu
KIDNEY CANCER
What is Kidney Cancer?
Renal Cancer (Adenocarcinoma)
Tumors of Renal Pelvis (Transitional Epithelial Cell Carcinoma)
There are two most common types of kidney cancers. Adenocarcinoma, which accounts for approximately 85% of kidney cancers is a type of cancer that starts in the tubules found in the kidney tissue (this will be explained below with details). And the other type begins in the basin-like part of the kidney (Renal pelvis, Image-1), where the kidney collects the urine.
Renal Cancer (Adenocarcinoma) starts in the small urine-carrying tubes found in kidneys.
Renal cancer (Renal Cell Cancer – RCC-, adenocarcinoma) originates in the epithelial cells lining the inner surfaces of small urine-carrying tubes in kidney, called tubules (Image-1). There are two kidneys in human body. And in each kidney, there are total 1 million tiny filtering units. Wastes in the blood are filtered by these tiny filtering units. This fluid is either reabsorbed by body or its wastes are removed while passing through small tubes in the kidney. And in the end, final product – the urine we discharge from our body – is produced. The urine produced is drained into the renal pelvis through urine-collecting renal calyces; and after that via canals named ureter it is drained into bladder where it will be stored for some time.
What is Kidney Cancer ?
While adenocarcinoma, which is also called renal cancer (Renal Cell Cancer, RCC) , starts in the tiny urine tubes (tubules), another form of it can also develop which originates in renal pelvis and ureter, called transitional epithelial cell cancer.
National Cancer Institute expects 79.000 new kidney cancer cases to be diagnosed in USA in 2022. Number of patients who will lose their lives due to kidney cancer is also predicted as 13.920 for the same year.
5-year relative survival rate between 2012-2018 is 76.5%
RCC occurs both sporadic and heritable forms.
Four RCC syndromes with autosomal dominant inheritance have been described as i.) Von Hippel Lindau Disease (VHL) ; ii.) Hereditary Leiomyomatosis and Renal Cell Cancer (HLRCC) ; iii.) Hereditary papillary Renal Carcinoma (HPRC) ; iv.) Birt-Hogg-Dube Symdrome (BHD).
The history of each RCC is distinct and influenced because of several factors, consisting o histologic features and genetic alterations.
Young age at RCC onset is also a clue that hereditary etiology is possible. In contrast with sporadic RCC, which is generally diagnosed during the 5th to 7th decades of life.
Hereditary RCC from NCI, the median age of RCC diagnosis was 37 years, with 70% of patients being diagnosed at age younger than 46.
Heritable RCCS are often multifocal and bilateral.Patients with sporadic RCC who underwent genetic testing revealed that 6.1 of population had positive genetic test results, 75% has negative.
Smoking and overuse of painkillers increase the risk of developing kidney cancer.
Smoking
Overuse of painkillers for a long period of time
Genetic (hereditary) risk
For instance: von Hippal Lindau syndrome or renal cancers such as hereditary papillary renal cell carcinoma can be defined.
Most common clinical symptoms we come across in patients with renal cancers are blood in urine and palpable solid mass in abdomen noticed during physical examination. In addition to blood in urine and a noticeable mass in abdomen, it frequently causes additional symptoms. Renal cancers in early stages are often asymptomatic. And diagnoses of these patients are generally made coincidentally while they are undergoing ultrasonography or other radiological procedures for some other reasons.
Those who have below mentioned symptoms should be evaluated in terms of renal cancer:
Blood in urine
A solid, palpable mass in abdomen
Chronic kidney pain
Loss of appetite
Weight loss
Anemia
Abdomen and kidneys have to be examined in order to diagnose and evaluate renal cancers.
These examinations/tests are:
Physical Examination and family history:
Is there a family history of kidney cancer? Are there any other risk factors? Is there a palpable mass in the abdomen?
Blood analysis:
Are there any additional symptoms to accompany kidney cancer? Such as anemia, hyperchromasia, high calcium in blood, abnormality in liver functions.
Urinalysis:
Is there blood in urine?
Ultrasonography:
Ultrasonographic evaluation of kidneys is the most important diagnostic procedure to be performed in the first place. The final definition of the suspicious mass (Image-2) is made generally with Doppler ultrasonography, or ideally with computed tomography or magnetic resonance (MR) imaging (Image-3a and -3b).
Image-2: View of the suspicious mass in kidney
Renal tumor
How is kidney cancer diagnosed?
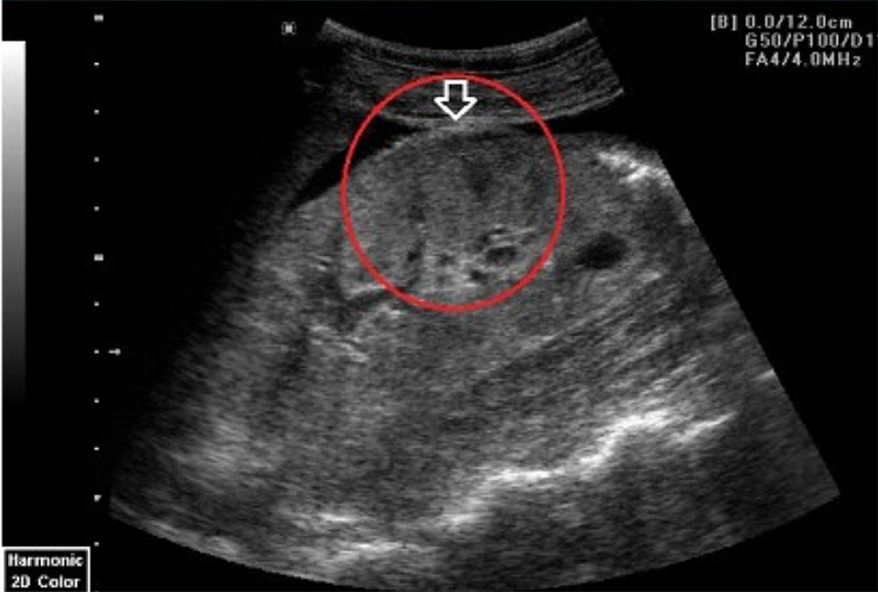
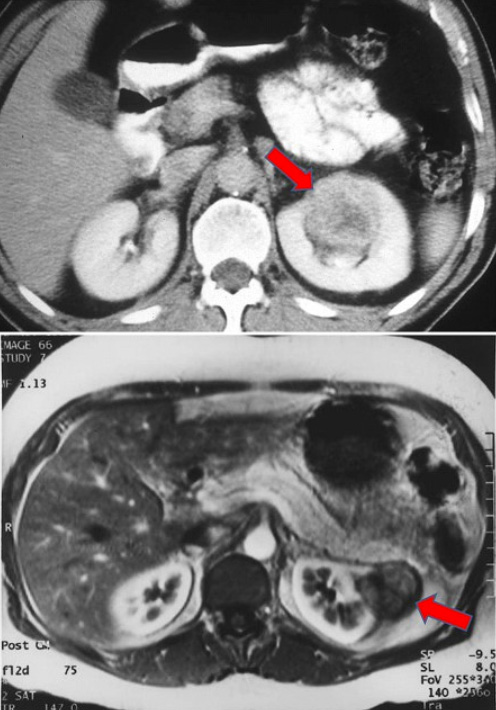
Image-3a and -3b: Renal cancer masses (pointed with red arrows) detected on images provided by computed tomography (3a) and MRI evaluations (3b).
Computed tomography:
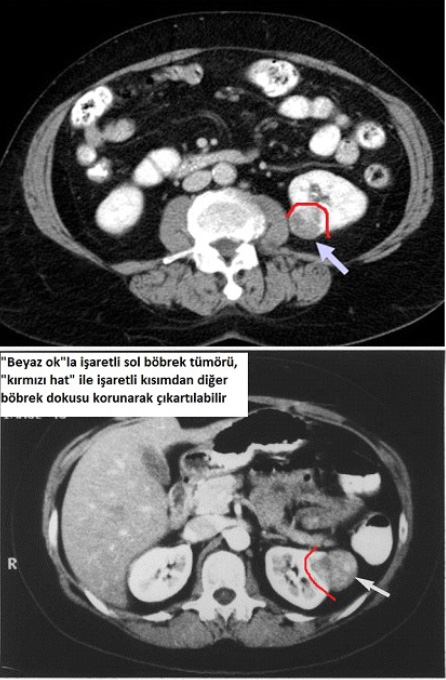
Provides simultaneous cross-sectional evaluation of abdominal organs. In addition to that, thanks to the intravenously injected contrast material, we can see whether the renal mass contrast retention exists or not and have an idea about the vascular structures feeding the mass. Besides, localization of the mass in the kidney and its sizes can be certainly identified, which are very important details for the surgery to be planned. Structural shape of renal arteries and veins (only a single renal artery?, any anatomical differences?), their courses and their connections with tumor (which branch[es] of the renal artery reaches the tumor) are very important points. In case of a localized tumor mass which do not have a close connection with renal artery and renal vein, it is very important to remove the mass while preserving the remaining health part of kidney (Image-4).
3-Dimensional Computed Tomography – Angiography:
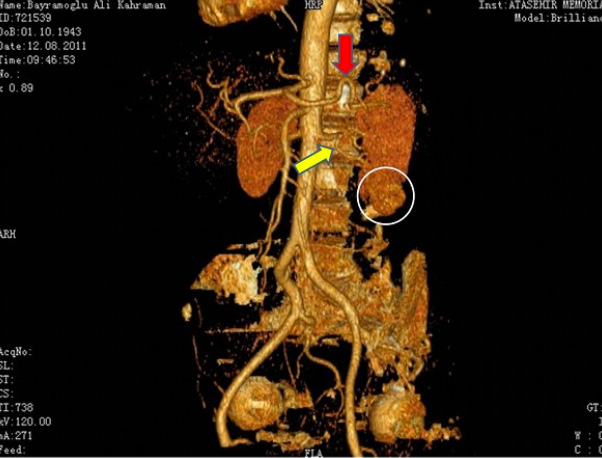
Thanks to this evaluation procedure, 3-dimensional images of kidney, its arteries, veins, and the tumor can be obtained with a special technique (Image-5). I carry out this evaluation especially for the patients that I plan to perform Laparoscopic and Robotic partial nephrectomy (which is excising only the tumor and leaving the healthy kidney tissue in), most particularly for whom I do not plan to clamp the renal artery completely. By this mean, we become able to evaluate the pre-operative conditions of the vascular structures, how and from which level they enter the kidney, their courses in the kidney and their connections with tumor tissue; and this evaluation allows us to make a surgical plan.
Image-5:
3-dimensional evaluation of renal artery and the mass in the kidney (Red arrow: Renal artery located at the upper side of the kidney, Yellow arrow: Renal vein located at the lower side of the kidney – its lower branch reaches the mass –, White circle: the mass located in the lower part of the kidney)
3-Dimensional computed tomography in Kidney Cancer
MR Imaging:
It is subsidiary in diagnosing and evaluating the above-mentioned connections of tumor with vascular structures, especially in some of the cases for whom computed tomography cannot be used.
Biopsy:
In some cases, this procedure can be used in case of a suspicion about the diagnosis. It is performed under computed tomography guidance. However, in pathologic evolution biopsy plays a limited role in making the true diagnosis. The most significant reason is that the material removed for pathologic evaluation is generally insufficient, so the precision of diagnosis is questioned.
Today, thanks to early diagnosis methods, renal tumors can be detected at very early stages while they are still small in size. So ‘’partial nephrectomy’’, during which the kidney can be preserved at maximum level and only the cancerous tissue is excised, has gradually gained importance.
Prof. Dr. Tibet Erdogru can perform laparoscopic surgical removal of the renal tumors up to 6cm in size without clamping renal artery and renal vein, without restricting the blood supply of kidneys (which is called ‘’unclamped renal pedicle’’ in medical literature).
In order to watch the video of laparoscopic partial nephrectomy operation performed without using ‘’Renal Pedicle Clamping’’ and blocking the blood flow to kidneys, please CLICK HERE.
In 5 and 10 years of follow-ups carried out for scientific researches, in terms of cancer survival and tumor recurrence rates there is no difference between conditions of patients who underwent ‘’Partial Nephrectomy’’ (which is removal of only the cancerous tissue and leaving the healthy tissue in) and who underwent a surgery for total removal of kidney (provided that the compared patients have the same cancer stages – stage T1, in which tumor is smaller than 7cm).
There are some factors affecting prognosis (life expectancy by taking into consideration the disease) and the type of the treatment to be applied.
Most important factors are;
- Stage of the disease
- Patient age and general state of health
Cancer stating system is used in order to find out the clinical condition of the kidney cancer and the course of the disease easily, and to plan the treatment. Leading parameters of this staging system is the size of the tumor, its connection with the kidney and surrounding tissues, and whether it has spread to any distant tissues or not. In treatment of renal cancers with large tumor sizes (Image-6) and distant organ metastasis, open surgery can be preferred to laparoscopic surgery.
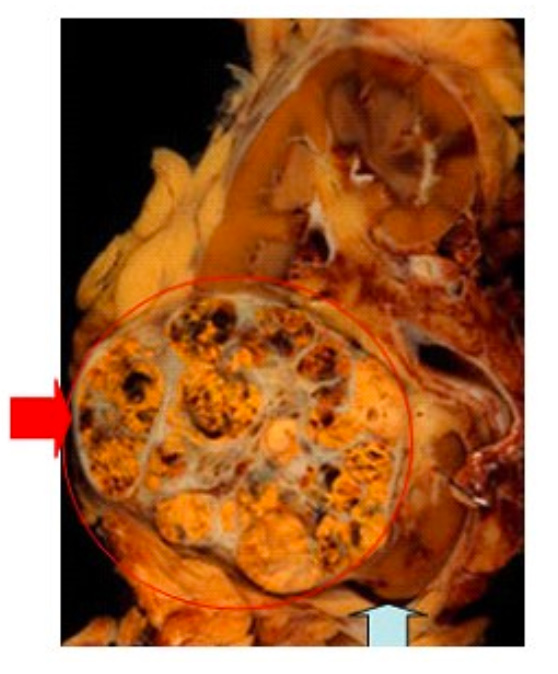
Image-6: Image of a renal cancer which is very extended and in an advanced stage in terms of tumor size (red circle pointed with red arrow), and normal kidney tissue (blue arrow)
However, as stated above, even for large renal tumors limited to kidney just like the one in Image-7, tumors that size up to 10-15 cm can also be removed laparoscopically (depending on surgeon’s experience). Nowadays laparoscopy is accepted as the gold standard for these kinds of masses.
Image-7: Renal adenocarcinoma limited to renal capsule but not suitable for only partially removal of tumor because of its size and localization. Today, ‘’laparoscopic’’ technique is accepted as the suitable treatment type for a tumor with these features.
Tumors of Renal Pelvis (Transitional Epithelial Cell Carcinoma)

As it can be seen in the image on the right, urine is drained into renal pelvis through yellow colored tubes and it is carried into bladder via the urinary canal called ureter. Urine collected in bladder is stored there until removed from body with urination.
The type of cancer that is called transitional epithelial cell carcinoma originates in the epithelium layer lining the inner surface of this above-mentioned structure. For this reason, types of the cancers formed in bladder and renal pelvis are the same.
Since it also occurs in kidney, it is presented to you with kidney cancers too, for informational purposes.
These types of cancers are called tumors of renal pelvis.
Tumors of Renal Pelvis
Transitional epithelial cell carcinoma develops from structural degenerations of ‘’transitional epithelial cells’’ that line the inner surfaces of ureters and renal pelvis. This is also called ‘’Urothelial Carcinoma’’.
Transitional epithelial cell cancer of renal pelvis accounts for around 72% of all kidney cancers. If the tumor is detected at an early-stage and it is in the primary phase, treatment chances are higher than 90%. However, in case of a cancer growth into deep muscle layer, chance for curing the disease may fall to a rate around 15%, even if the cancer is limited to renal pelvis and ureter (has not spread outside the tissue border).
Most common reasons that are known
- Overuse of painkillers for long periods of time
- Direct exposure to dyes and chemicals used in plastic, leather and tire industries
- Smoking
Clinical symptoms we encounter the most
- Blood in urine accompanied by pain/or without any pain
- Low back pain
In case of having below-mentioned complaints and problems, one should visit a doctor.
- Blood in urine (even if it has happened for once, visiting a doctor is necessary)
- Chronic left or right low back pain
- Severe exhaustion
- Weight loss with no reason
- Painful and frequent urination
Patients consulting with these reasons must be evaluated in detail.
Physical Examination
Urinalysis: Blood presence should be seen in urine.
Ultrasonography: A dilation related to urine canal blockage caused by kidney tumor might be present. Or a mass can be seen in the kidney.
IVP: Despite being the previous standard diagnosis procedure, intravenous pyelography (a radiologic exam that uses injection of contrast material) is a method that is still frequently used today. This radiologic test shows very important signs regarding especially renal pelvis and ureter tumors.
Computed Tomography: In addition to providing information about the size of the mass and whether the mass in renal pelvis or ureter has spread into surrounding tissues, it also offers an opportunity to see presence of an unexpected spread of disease to liver and lymph nodes.
Ureteroscopy: During this procedure, an endoscopic device (which is usually a flexible ureteroscope) is inserted into the urine canal called ureter, then renal pelvis and all the small calyces within the renal pelvis are checked. Biopsy samples may be taken when necessary.
Treatment of Kidney Cancer
After the diagnosis is made, there are some factors affecting the prognosis (chances of cure). Treatment option can be discussed with patient in consideration of these factors. First two factors affecting the prognosis in the first step are the stage of tumor, and ‘’grade’’ of tumor cells.
Top four questions to be asked:
- What is the stage and grade of tumor?
- Where is the tumor located?
- What are the medical conditions of patient and the other kidney?
- Is it recurrent cancer?
If the diagnosis is made at an early stage without being late, most of the transitional epithelial cell carcinomas of renal pelvis and ureter can be totally cured.
While most of the superficial transitional epithelial cell cancers are in low-grades, the tumors that have spread into deeper layers are high-grade tumors.
Possibility of having the same kind of a tumor in the second kidney is between 2-4% (at the same time or in another time). However, for the cases diagnosed with renal pelvis or ureter tumors, possibility of being diagnosed with that kind of a tumor in bladder simultaneously or in the future is between 30-50%.
Prof. Dr. Tibet Erdogru
Treatment of prostate, bladder, kidney and testicular cancers with robotic and laparoscopic surgery in urology
Our Clinic

- Hacı adil cad. Zerrin sokak, No:2/2 Levent, 34330 Beşiktaş İstanbul Turkey
Prof. Dr. Tibet Erdoğru – Urology & Robotic Surgery | Data Privacy | Cookie Policy